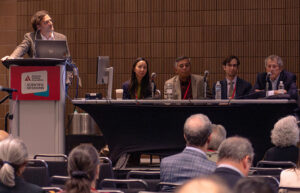
Who has been counted and who has been missed among ethnic and racial populations in the United States—and how this affects research needs and clinical care—took center stage during the 2026 Scientific Sessions panel discussion, Mapping Diabetes: Epidemiology in a Changing U.S. Demographic Landscape, held on Friday, June 5.
“Would you rather be missed or misunderstood? I would rather be misunderstood so that I can explain. But if you are missed and you are invisible, then that door is closed—you can’t talk about possibilities,” said Florence Hoffert-Dallo, PhD, MPH. “For decades, Middle Eastern and North African (MENA) populations have not been included in federal registry systems, so it makes it really difficult to understand the burden of diabetes as it relates to this population.”
Dr. Hoffert-Dallo, Chairperson and Professor of Public Health at Oakland University, focused her presentation on the dearth of health data specific to MENA populations in the United States, which she connected to several factors, including the fact that it was not until March 2024 that the U.S. Office of Management and Budget designated MENA as a separate category (including for the upcoming 2030 federal census).
On-demand access to recorded presentations from this and other sessions will be available to registered participants following the conclusion of the 2026 Scientific Sessions, from June 10–August 10.
Without federal census data, researchers used an array of primary data, surname algorithms, and other information to estimate diabetes incidence among MENA populations in the United States, with estimates varying widely, from 1.5–24%.
“We’ve lost all this time and all this data and don’t really understand the burden of diabetes in this community, which has led to greater mortality, higher complications, and other things that could have been prevented,” Dr. Hoffert-Dallo said.

She recommended that future research prioritize estimating a baseline level of diabetes prevalence among MENA populations in the United States.
Jithin Sam Varghese, PhD, MTech, Assistant Professor in the Hubert Department of Global Health and Emory Global Diabetes Research Center at Emory University, focused on the challenges of establishing and interpreting diabetes rates among Asian populations in the United States.
He noted that understanding the burden of diabetes among these populations has been challenged by a decline in self-reporting, significant undiagnosed diabetes, a lack of oversampling in the key National Health and Nutrition Examination Survey, and the fact that some 40% of all Asian Americans live in California, with the vast majority of published subnational estimates across Asian ethnic subgroups based on cohorts or electronic health record (EHR) data from that state.
Dr. Varghese said some of these challenges could be resolved by creating and accessing larger data sets. He pointed to ongoing research tapping nationwide electronic health records combined with cross-walking data on the national distribution of ethnic groups, which should assist with this.
Looking forward, Dr. Varghese said it would be important to track whether the burden of diabetes is increasing and whether the rate of prediabetes is flat among Asian American subgroups, and that “national efforts should be made to improve rates of screening among Asians who self-report prediabetes.”
Sherita Hill Golden, MD, MHS, the Hugh P. McCormick Family Professor of Endocrinology and Metabolism at Johns Hopkins University School of Medicine, turned her attention to the diabetes burden among African Americans. She pointed to studies that have shown a dramatic increase in the prevalence of diabetes among non-Hispanic Black Americans compared to other racial and ethnic groups.
Dr. Golden noted the reasons for these disparities lie in a complex web of historic inequalities and structural racism, from residential redlining and healthcare professional bias to sustained prescription disparities. For example, she noted a Veterans Health Administration meta-analysis of more than 14.6 million patients that indicated Black individuals receiving care had 20% lower odds of receiving a sodium-glucose cotransporter-2 inhibitor (SGLT2i) or glucagon-like peptide-1 receptor agonist (GLP-1 RA).
Dr. Golden said data-proven academic-community partnership models are emerging to address some of these disparities. The most successful ones, she noted, use culturally tailored education and empowerment with direct patient engagement, which includes taking racial and ethnic groupings into account.
“It’s important to allow people to identify themselves so we can understand who we are treating and how we need to adapt that treatment. During COVID-19, I think it became very clear when we initially did not have all that data in our health systems, and so we did not know who was dying disproportionately and where we needed to target our testing,” Dr. Golden said. “But beyond knowing who we are targeting, we have to keep people at the center—people like feeling seen.”

Save the date
Make plans to join us June 18–21, 2027, for the 2027 Scientific Sessions at the Walter E. Washington Convention Center in Washington, DC. Registration will open in January.